Sunday, 19 November 2017
Lanre Jacob Sarcoma Foundation: HOW GENETIC TESTING CAN PREVENT INHERITED CANCERS
Lanre Jacob Sarcoma Foundation: HOW GENETIC TESTING CAN PREVENT INHERITED CANCERS: HOW GENETIC TESTING CAN PREVENT INHERITED CANCERS SUCH AS BREAST,OVARIAN, COLORECTAL AND PROSTATE CANCERS. Genetic testing also ...
HOW GENETIC TESTING CAN PREVENT INHERITED CANCERS
HOW GENETIC TESTING CAN PREVENT INHERITED CANCERS SUCH AS BREAST,OVARIAN, COLORECTAL AND PROSTATE CANCERS.
By Maryam Ajikobi

Genetic testing also known as DNA testing allows the determination of blood lines and the genetic diagnosis of vulnerabilities to inherited diseases.
To prevent or treat some hereditary cancers,
taking a patient’s full family health history is critical. When there is a
strong history of breast, ovarian, pancreatic, colon or prostate cancer in a
family, other members are predisposed, and it will be important to have a
genetic testing done to know if a person has inherited the gene that causes the
inherited cancer. For instance, mutations in the BRCA genes are well-known
genetic variants that can predispose a person to cancers that include breast,
ovarian and prostate.
When physicians and genetic counselors have genetic and family information, they can guide patients on more precise prevention recommendations and treatment decisions. Genetic factors and family history can help inform when a man should be screened for prostate cancer, or when a biopsy to check for prostate cancer is a good idea. It can guide decisions on when a woman should start her mammogram screening and whether additional screening with an MRI is warranted. When cancer is detected, testing of the cancer’s genetic make-up can help doctors determine whether immediate treatment is necessary and the types of interventions that are likely to be most effective.
RISKS ASSOCIATED WITH INHERITED CANCERS. Your risk of having prostate cancer is doubled if your father or brother had prostate cancer. Your risk also depends on the age at which your relative was diagnosed. Men whose families carry the gene changes that cause breast cancer, BRCA1 or BRCA2, are thought to be at increased risk for prostate cancer.
When physicians and genetic counselors have genetic and family information, they can guide patients on more precise prevention recommendations and treatment decisions. Genetic factors and family history can help inform when a man should be screened for prostate cancer, or when a biopsy to check for prostate cancer is a good idea. It can guide decisions on when a woman should start her mammogram screening and whether additional screening with an MRI is warranted. When cancer is detected, testing of the cancer’s genetic make-up can help doctors determine whether immediate treatment is necessary and the types of interventions that are likely to be most effective.
RISKS ASSOCIATED WITH INHERITED CANCERS. Your risk of having prostate cancer is doubled if your father or brother had prostate cancer. Your risk also depends on the age at which your relative was diagnosed. Men whose families carry the gene changes that cause breast cancer, BRCA1 or BRCA2, are thought to be at increased risk for prostate cancer.
Your risk of having ovarian cancer is doubled if
your first-degree relatives (mother, daughter, sister), especially if two or
more have had the disease. A family history of breast or colon cancer also is
associated with an increased risk of developing ovarian cancer. Women who have
had breast or colon cancer may be at greater risk.
If you’ve had breast cancer in one breast, you have an increased risk of developing cancer in the other breast. If your mother, sister or daughter was diagnosed with breast cancer, particularly at a young age, your risk of breast cancer is increased. Still, most of, many of people diagnosed with breast cancer have no family history of the disease. Certain gene mutations that increase the risk of breast cancer can be passed from parents to children. The most common gene mutations are referred to as BRCA1 and BRCA2. These genes can greatly increase your risk of breast cancer and other cancers, but they don’t make cancer inevitable.
If you’ve had breast cancer in one breast, you have an increased risk of developing cancer in the other breast. If your mother, sister or daughter was diagnosed with breast cancer, particularly at a young age, your risk of breast cancer is increased. Still, most of, many of people diagnosed with breast cancer have no family history of the disease. Certain gene mutations that increase the risk of breast cancer can be passed from parents to children. The most common gene mutations are referred to as BRCA1 and BRCA2. These genes can greatly increase your risk of breast cancer and other cancers, but they don’t make cancer inevitable.
HOW
TO PREVENT THIS FROM HAPPENING
Get a genetic testing done today, visit http://humgene.com/services/genetic-testing/.You can discuss with a genetic counsellor if you are not sure of what to do (send your enquiry to info@humgene.com).
Get a genetic testing done today, visit http://humgene.com/services/genetic-testing/.You can discuss with a genetic counsellor if you are not sure of what to do (send your enquiry to info@humgene.com).
OTHER
BENEFITS OF GENETIC TESTING
Genetic testing helps to identify people who are more prone to develop a medical condition that may be preventable. For example, asymptomatic people with the BRCA gene mutation (Harmful mutations in these genes may produce a hereditary breast-ovarian cancer syndrome in affected persons) may opt to remove their breasts and ovaries as a prophylactic measure (preventive or protective measure).
Similarly, individuals with a family history of familial adenomatous polyposis (an inherited disorder characterized by cancer of the large intestine (colon) and rectum) have been saved by colonoscopy (a procedure in which a trained specialist uses a long, flexible, narrow tube with a light and tiny camera on one end, called a colonoscope, passed through the anus to look inside your rectum and colon) and removal of growths in the colon or by colostomy (a surgical procedure to remove all or part of the colon). A smoker, with a cardiac family history, is cautioned well in advance to modify his lifestyle.
Genetic testing helps to identify people who are more prone to develop a medical condition that may be preventable. For example, asymptomatic people with the BRCA gene mutation (Harmful mutations in these genes may produce a hereditary breast-ovarian cancer syndrome in affected persons) may opt to remove their breasts and ovaries as a prophylactic measure (preventive or protective measure).
Similarly, individuals with a family history of familial adenomatous polyposis (an inherited disorder characterized by cancer of the large intestine (colon) and rectum) have been saved by colonoscopy (a procedure in which a trained specialist uses a long, flexible, narrow tube with a light and tiny camera on one end, called a colonoscope, passed through the anus to look inside your rectum and colon) and removal of growths in the colon or by colostomy (a surgical procedure to remove all or part of the colon). A smoker, with a cardiac family history, is cautioned well in advance to modify his lifestyle.
Maryam Ajikobi, A Sr. wrote this article for
Lanre-Jacob Savcoma Cancer Foundation on request. She is a Human Geneticist and
Counselor, trained in McGill University, Canada. She is currently a PhD
Candidate Public Health and Epidemiology. She is passionate on how to prevent
Genetic Disorder and diseased, especially inherited cancers such as breast,
ovarian, prostate and colorectal cancers. She is the CEO of HumGene Limited,
the first Genetic testing company in Nigeria.
Website: www.humgene.com
Instagram: www.instagram.com/humgenelimited/
--------------------------------------------------------
Website: www.humgene.com
Instagram: www.instagram.com/humgenelimited/
--------------------------------------------------------
References
Brown, J., Jhingran, A., Deavers, M., et al. Stromal tumors of the ovary. Raghavan, E., Brecher, M. L., Johnson, D. H., et al. (Eds.). (2006). Textbook of Uncommon Cancer. (3rd Edition). Chichester, England: John Wiley & Sons. 41: pp. 455-466Matei, D. E., Schilder, J. M., & Michael, H. Germ cell tumors of the ovary. Raghavan, E., Brecher, M. L., Johnson, D. H., et al. (Eds.). (2006). Textbook of Uncommon Cancer. (3rd Edition). Chichester, England: John Wiley & Sons. 42: pp. 467-476.
“SEER Stat Fact Sheets: Breast Cancer”. NCI. Retrieved 18 June 2014.
“Prostate Cancer”. National Cancer Institute. Retrieved 16 July 2016.
www.usnews.com
Saturday, 18 November 2017
Prostate Cancer and Nigerian Men
On Prostate Cancer and Nigerian Men
By Motolani Ogunsanya, B. Pharm., PhD

One out of seven men reading this will be diagnosed with prostate cancer in their lifetime. Prostate cancer is one of the most highly diagnosed cancers and the leading cause of cancer deaths among men in Nigeria. Similar to the rates seen in Black men from other populations, Nigerian men present with a higher stage and grade of prostate cancer and often the more aggressive ones.
Prostate cancer screening still remains the best available method of detecting prostate cancer early. There are two tests that are used to detect prostate cancer: the prostate-specific antigen (PSA) and the digital rectal examination (DRE) test. The PSA test measures the level of PSA, a protein produced by cells of the prostate gland, in the blood. The DRE test involves checking (or palpating) the surface of the prostate gland for bumps, hard spots, and any other abnormalities.
Some of the risk factors for prostate cancer include increasing age, being male, positive family history of prostate cancer, ethnicity (being Black or African), and lifestyle (poor diet and lack of exercise). Prostate cancer may not produce symptoms in its early stages. As a result, you may look healthy or even feel fine, and not know that there is a problem. If signs and symptoms are present, they may include: – blood in the urine; – the need to urinate frequently, especially at night; – weak or interrupted urine flow; – pain or a burning feeling while urinating; – inability to urinate; and – regular pain in the lower back, pelvis, or upper thighs.
When detected early, prostate cancer can be treated in time, and the chances of surviving are higher. If your risks are high already, a simple test can reduce the burden of complicated (palliative) treatment and the toll it takes on you and your loved one. However, prostate cancer screening rates are low among Nigerian men. There are many speculated reasons for this, which are not uncommon with Black men from other parts of the world. First, the practice of seeking proactive, preventative health measures, such as prostate cancer screening is not a common practice among men, especially Nigerian men. Low level of awareness about prostate cancer and its risk factors are also some of the speculated reasons for low screening rates. The invasiveness of the test (especially the DRE) has been reported to be a deterrent to undergoing screening.
Prostate cancer screening is not also without its disadvantages. The tests are not always specific enough to detect prostate cancer. As a result, this can result in over-diagnosis especially of cancers that may not have led to clinical problems if they had been left untouched. In addition, the use of aggressive therapy on such cancers is associated with unnecessary risks of urinary, sexual and bowel dysfunction, which have been shown to significantly impact quality of life. Other factors include fatality, masculinity, and stigma. Men have been reported to visit their doctors less than women, and are often embarrassed to discuss their health issues. Statistically, one out of four men did not visit a doctor in the past twelve months. As a result, prostate cancer is often diagnosed at later stages, when the odds of survival are low. The good news, however, is that if detected early, prostate cancer is often treatable and curable.
So, who should get tested?
- From age 50 onwards, discuss having a prostate checkup with your doctor.
- If there is a family history of prostate cancer, then a checkup should form part of your general checkup from age 40.
- Any time you experience any urinary symptoms, get a checkup.
Unfortunately, cancer, especially, prostate cancer still remains heavily stigmatized in Nigeria. To achieve a healthier nation, we need to begin to talk more comfortably about reducing the stigma associated with cancer. It does not bode us well to keep suffering in silence, especially when help is often around the corner. It’s November - prostate cancer month, and I’d like to use this as a medium to promote prostate health. While prostate cancer screening is not for everyone, it is essential to discuss your risk factors and susceptibility to this disease with your doctor. I would also like to urge the women (mothers, daughter, sisters, aunts, cousins, nieces, etc.) in these men’s lives to talk to them and remind them to get their yearly examinations done and also assess their prostate cancer risk.
For peace of mind, yours and your loved ones’, the first step to preventing prostate cancer deaths is early detection. This begins by first talking to your doctor.
Dr. Ogunsanya, an Associate Professor, writes for LJSCF from Oklahoma University. She is passionate about cancer
advocacy and reducing cancer incidence rates. Dr. Ogunsanya's research focuses on health economics and
outcomes research using mixed methodologies. Her research interests primarily
involve understanding health behaviors among underserved, minority groups and
the use of patient-reported outcomes to capture disease burden in patients with
rare diseases, cancer, and other disease conditions. Additional research
interests include examining quality of life through theoretical frameworks and
large-scale retrospective database analyses.
LinkedIn: https://www.linkedin.com/in/motolani/References
Center for Cancer Prevention & Control Prevention and Health Promotion Administration Maryland Department of Health & Mental Hygiene, April 2013
Groenwald S. Cancer Nursing: Principles and Practice. Philadelphia, PA: Jones and Bartlett Publishing; 2000.
Kanaan ZM, Eichenberger MR, Ahmad S, et al. Clinical predictors of inflammatory bowel disease in a genetically well-defined Caucasian population. Journal of negative results in biomedicine. 2012;11:7.
National Cancer Institute. Cancer Trends Progress Report – Costs of Cancer Care 2020. http://www.cancer.gov/newscenter/newsfromnci/2011/CostCancer2020. Accessed October 14, 2013. Odedina FT, Akinremi TO, Chinegwundoh F, et al. Prostate cancer disparities in Black men of African descent: a comparative literature review of prostate cancer burden among Black men in the United States, Caribbean, United Kingdom, and West Africa. Infectious agents and cancer. 2009;4 Suppl 1:S2.
Ogunsanya ME, Brown CM, Odedina FT, Barner JC, Corbell B, Adedipe TB. Beliefs Regarding Prostate Cancer Screening Among Black Males Aged 18 to 40 Years. American journal of men's health. 2016. Ogunsanya ME, Brown CM, Odedina FT, Barner JC, Adedipe TB, Corbell B. Knowledge of Prostate Cancer and Screening Among Young Multiethnic Black Men. American Journal of Men's Health.0(0):1557988316689497.
The Black Population: 2010. 2011; http://www.census.gov/population/race/. Accessed October 24, 2013. Wilt TJ, MacDonald R, Rutks I, Shamliyan TA, Taylor BC, Kane RL. Systematic Review: Comparative Effectiveness and Harms of Treatments for Clinically Localized Prostate Cancer. Annals of internal medicine. 2008;148(6):435-448.
Friday, 3 November 2017
A Cancer Education with Passion: How we do it…
The Preventive Cancer
Care Project is a grassroots program passionately carried out through
cancer education at Primary Healthcare Centers and in communities. We also
organize cancer education for artisans, students (Primary, secondary and higher
institutions), the military, and at religious places.
In
addition, customized seminars/workshops are organized for families and
corporate bodies while we also educate the people via radio, printing of flyers
& banners, mouth to mouth campaign, and the social media.
OUR RESOURCE PERSONS
Our
resource persons are cancer experts drawn from our partner institutions such as
the Lagos State Ministry of Health, Lagos University Teaching Hospital (LUTH),
the Lagos State Primary Health-care Board, etc.
OUR CENTRAL MESSAGE

Our
message is centered around causes of cancer, symptoms, cancer treatment
options, need for healthy lifestyle changes (including healthy dietary
choices), regular cancer tests/screenings for prevention and for early
detection, etc.
Starting From Lagos, Nigeria


The LJSCF’s Preventive Cancer-care
Advocacy was
launched in
Lagos, and is
gradually spreading to other parts of Nigeria.
Through
our recent collaboration with Lagos State Ministry of Health and the Lagos
State Primary Health Care Board, LJSCF now has access to carry out cancer
education (including cancer screenings/tests) in about 300 Primary Health-care
centers, and in all communities in Lagos state.
This means that we have a huge
population of about 20 million people to educate, both in the urban and the
rural parts of the state.
With the active support of our partners
and donors, we hope to
launch our Health & Safe
Water Project soon, as part of our Preventive Cancer Care Project,
in Lagos State and other parts of Nigeria.
Monday, 21 August 2017
Cancer Situation in Nigeria

Deaths from Cancer, which cuts across the rich and the poor,
is increasing at alarming rate in
Nigeria. Yet, most Nigerians, especially at the grassroots, are not only
ignorant about cancer causes, symptoms, and how it can be prevented, majority
do not even know about the need to go for regular cancer tests/screenings.
Therefore, apart from
provisions of support for cancer patients and rehabilitation for cancer
survivors, LJSCF’s adopted the Preventive Cancer-care policy, which helps us to focus our energy more on cancer education
and life-saving projects (such as provision of safe water, etc) that can help
our cancer prevention goal. Our focus is not only in the urban centers, but
especially, in rural communities across Nigeria.
Support Our Preventive Cancer Care Project in Nigeria1
Since you’re here …
… we have a small favour to ask. More people are reading information about cancer that we share on this blog... BECOME OUR SUPPORTER
LJSCF’s aim is
to make the world a better, fair place; we want to keep the policy makers
committed to improving the health of the people. We want to help the people
adopt healthy lifestyles that help lower the risk of cancer.
Doing this means
keeping the society informed about cancer and other related health issues. This
is not only essential for the health of the people, but for the productivity
and the development of our country.
Like many
other nonprofit organizations, LJSCF is operating in an incredibly challenging
financial climate. Our founder, Lanre Jacob, a survivor of a thirty-year cancer
experience, is not a wealthy man pulling the strings.
Having
survived, Lanre Jacob’s passion is to help millions of people in Nigeria escape
death from cancer through sustained cancer education in every part of Nigeria,
and through every medium possible.
In addition to
this is caring for cancer patients and cancer survivors. Our aim is to provide modern
rehabilitation centers for cancer survivors, so they can also live productive
and fulfilled lives.
We know that not everyone is in a position to become a
Supporter. But if you can, you’ll be an integral part of our mission to make
the world a better, fairer place, for everyone.
Make the future more secure and better for everyone by supporting our Foundation.
Glutathione Foods
What Foods
Promote the Highest Glutathione Levels?
Many whole
foods contain significant amounts of glutathione or its precursors. Foods
richest in sulfur-containing amino acids are usually the best sources of
glutathione:
·
The overall top food for maximizing your glutathione is high
quality whey protein. It must be cold pressed whey protein derived from grass
fed cows, and free of hormones, chemicals and sugar. Quality Gwhey provides all the key amino acids for
glutathione production (cysteine, glycine and glutamate) and contains a unique
cysteine residue (glutamylcysteine) that is highly bioactive in its affinity
for converting to glutathione. Glutamylcysteine is a bonded cysteine molecule
(cysteine plus glutamate) that naturally occurs in Bovine Serum Albumin – a
fragile immune component of the whey. This unique cysteine is exclusive to whey
and rarely appears in other protein foods – which makes whey protein the best
glutathione-promoting food source. Furthermore, whey provides critical
co-factors, immunoglobulins, lactoferrin and alpha Lactalbumin (also a great
source of cysteine), which together help create the right metabolic environment
for high glutathione activity.
·
Raw milk products, raw eggs and
meat: Glutathione occurs in the highest levels in fresh,
uncooked meats and raw milk, but is almost entirely absent in pasteurized dairy
products.
·
Fresh fruits and vegetables provide
excellent glutathione, but once cooked, values become negligible. Spinach,
potatoes, asparagus, avocado, squash, okra, cauliflower, broccoli, walnuts,
garlic and tomatoes have the highest glutathione per serving.
·
The herb milk thistle is an
excellent source of the antioxidant compound silymarin, which may help to
prevent glutathione depletion in the liver. Glutathione is crucial in the liver
for detoxification and can become depleted from acetaminophen (Tylenol),
alcohol consumption, and general toxic overload.
·
Curcumin may also
be useful for increasing glutathione levels.
Keeping your
glutathione levels up is a matter of increasing factors that boost your
glutathione and decreasing factors that lower it. The things that deplete your
glutathione the fastest are chemicals, toxins and sugar.
WHAT MUCH DO YOU KNOW ABOUT GLUTATHIONE?
GLUTATHIONE (GSH)
Glutathione
Glutathione
is the most important natural (endogenous) antioxidant and is found in almost
every cell of the body. It is vital for cell protection as well as for proper
cell function and is, therefore, absolutely essential for maintaining good
health. Glutathione levels are highest in cells of organs in the body that are
most susceptible to toxicity, such as the liver, kidney, lungs, heart, eyes,
skin and brain. Thus, glutathione protects against cell-generated oxygen and
nitrogen free radicals when produced in excess, and the free radicals produced
by exposure to radiation from ultraviolet light, x-, gamma- and cosmic-rays.
Glutathione
not only neutralizes free radicals and reactive oxygen compounds, but maintains
exogenous antioxidants such as vitamins C and E in their reduced (active)
forms. Through direct conjugation, glutathione detoxifies many environmental
carcinogens and toxic xenobiotic (foreign) substances. It also protects against
toxic/carcinogenic pollutants such as cigarette smoke, vehicular exhaust fumes,
and smoke-stack effluents.
Glutathione
is essential for the proper functioning of the endogenous antioxidant enzyme
glutathione peroxidase. Our cell membranes are made up of polyunsaturated
lipids or fats and are susceptible to damage by the reactive oxygen species
(ROS), especially the peroxide radicals. This damage can affect the cell from
getting proper nutrients or waste material out and if not functioning properly
will lead to cellular death. The enzyme glutathione peroxidase detoxifies lipid
peroxides (reactive by-product from oxidation of lipids by free radicals) and
glutathione is a needed co-factor for this enzyme.
Glutathione
is needed for the growth, reproduction and differentiation of lymphocytes and
is essential for a full functioning immune system. Glutathione also plays an
active role in a multitude of metabolic and biochemical reactions, such as DNA
synthesis and repair, protein synthesis, prostaglandin synthesis, amino acid
transport and enzyme activation. Thus, glutathione plays a fundamental role in
maintenance of optimal health.
The
medical and basic science literature describe the importance of glutathione in
many facets of cellular function, especially in maintaining the
reduction/oxidation (redox) balance of cells that can be compromised by
environmental toxins and the stresses of urban lifestyles.
Facts on Glutathione
·
Naturally produced by the body.
·
As we age our glutathione levels
start to decline.1
·
Low glutathione levels are
associated with chronic diseases.
·
Glutathione is found in higher
concentration in organs that are subject to high toxic exposure, such as the
liver, kidney, lungs, skin, eyes and ears.

YOU CAN WALK ON YOUR CHALLENGES AS JESUS WALKED ON THE SEA
Like Lanre Jacob, the man who trusted the Lord for his total healing fromn dermato-fibro-sarcoma, a tumor that grew severally on his head, and were removed through surgery, you also can trust God and know the power of healing through Jesus Christ.





Monday, 7 August 2017
Wednesday, 12 July 2017
Water & Cancer
Our Foundation is not just advocating for safe water for cancer prevention, we are also set to enter into partners and investors to provide scalable, safe and affordable water to the urban and the rural poor across Nigeria, through innovative business models.

Tuesday, 9 May 2017

Saturday, 15 April 2017
What Is Cancer?


A Collection of Related Diseases
Cancer is the name given to a collection of related diseases. In all types of cancer, some of the body’s cells begin to divide without stopping and spread into surrounding tissues.
Cancer can start almost anywhere in the human body, which is made up of trillions of cells. Normally, human cells grow and divide to form new cells as the body needs them. When cells grow old or become damaged, they die, and new cells take their place.
When cancer develops, however, this orderly process breaks down. As cells become more and more abnormal, old or damaged cells survive when they should die, and new cells form when they are not needed. These extra cells can divide without stopping and may form growths called tumors.
Many cancers form solid tumors, which are masses of tissue. Cancers of the blood, such as leukemias, generally do not form solid tumors.
Cancerous tumors are malignant, which means they can spread into, or invade, nearby tissues. In addition, as these tumors grow, some cancer cells can break off and travel to distant places in the body through the blood or the lymph system and form new tumors far from the original tumor.
Unlike malignant tumors, benign tumors do not spread into, or invade, nearby tissues. Benign tumors can sometimes be quite large, however. When removed, they usually don’t grow back, whereas malignant tumors sometimes do. Unlike most benign tumors elsewhere in the body, benign brain tumors can be life threatening.
Differences between Cancer Cells and Normal Cells
Cancer cells differ from normal cells in many ways that allow them to grow out of control and become invasive. One important difference is that cancer cells are less specialized than normal cells. That is, whereas normal cells mature into very distinct cell types with specific functions, cancer cells do not. This is one reason that, unlike normal cells, cancer cells continue to divide without stopping.
In addition, cancer cells are able to ignore signals that normally tell cells to stop dividing or that begin a process known as programmed cell death, or apoptosis, which the body uses to get rid of unneeded cells.
Cancer cells may be able to influence the normal cells, molecules, and blood vessels that surround and feed a tumor—an area known as the microenvironment. For instance, cancer cells can induce nearby normal cells to form blood vessels that supply tumors with oxygen and nutrients, which they need to grow. These blood vessels also remove waste products from tumors.
Cancer cells are also often able to evade the immune system, a network of organs, tissues, and specialized cells that protects the body from infections and other conditions. Although the immune system normally removes damaged or abnormal cells from the body, some cancer cells are able to “hide” from the immune system.
Tumors can also use the immune system to stay alive and grow. For example, with the help of certain immune system cells that normally prevent a runaway immune response, cancer cells can actually keep the immune system from killing cancer cells.
How Cancer Arises
Cancer is a genetic disease—that is, it is caused by changes to genes that control the way our cells function, especially how they grow and divide.
Genetic changes that cause cancer can be inherited from our parents. They can also arise during a person’s lifetime as a result of errors that occur as cells divide or because of damage to DNA caused by certain environmental exposures. Cancer-causing environmental exposures include substances, such as the chemicals in tobacco smoke, and radiation, such as ultraviolet rays from the sun. (Our Cancer Causes and Prevention section has more information.)
Each person’s cancer has a unique combination of genetic changes. As the cancer continues to grow, additional changes will occur. Even within the same tumor, different cells may have different genetic changes.
In general, cancer cells have more genetic changes, such as mutations in DNA, than normal cells. Some of these changes may have nothing to do with the cancer; they may be the result of the cancer, rather than its cause.
"Drivers" of Cancer
The genetic changes that contribute to cancer tend to affect three main types of genes—proto-oncogenes, tumor suppressor genes, and DNA repair genes. These changes are sometimes called “drivers” of cancer.
Proto-oncogenes are involved in normal cell growth and division. However, when these genes are altered in certain ways or are more active than normal, they may become cancer-causing genes (or oncogenes), allowing cells to grow and survive when they should not.
Tumor suppressor genes are also involved in controlling cell growth and division. Cells with certain alterations in tumor suppressor genes may divide in an uncontrolled manner.
DNA repair genes are involved in fixing damaged DNA. Cells with mutations in these genes tend to develop additional mutations in other genes. Together, these mutations may cause the cells to become cancerous.
As scientists have learned more about the molecular changes that lead to cancer, they have found that certain mutations commonly occur in many types of cancer. Because of this, cancers are sometimes characterized by the types of genetic alterations that are believed to be driving them, not just by where they develop in the body and how the cancer cells look under the microscope.
When Cancer Spreads
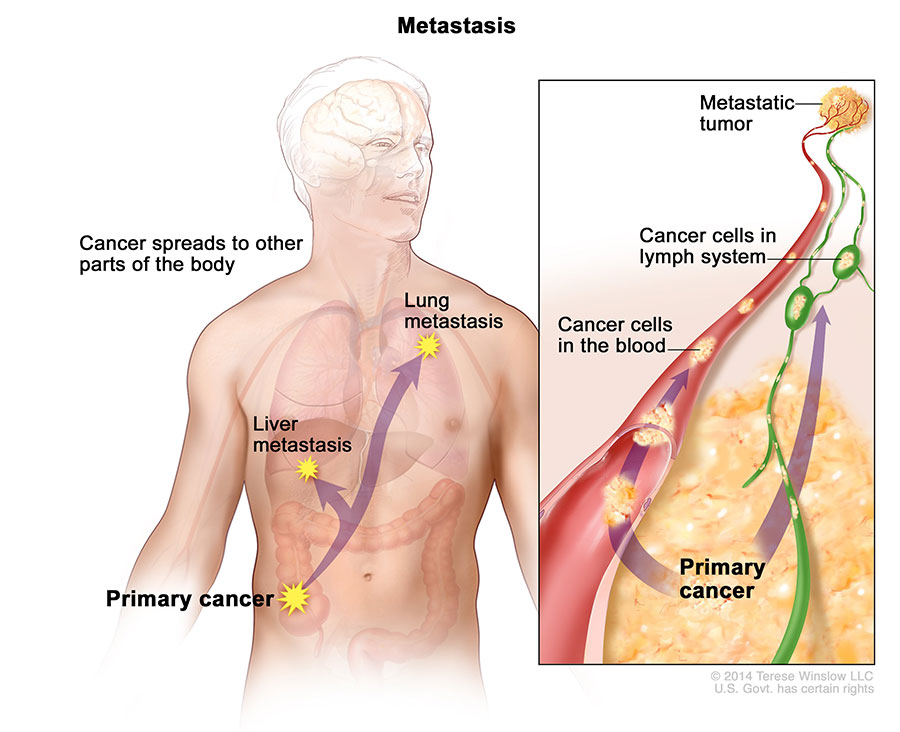
A cancer that has spread from the place where it first started to another place in the body is called metastatic cancer. The process by which cancer cells spread to other parts of the body is called metastasis.
Metastatic cancer has the same name and the same type of cancer cells as the original, or primary, cancer. For example, breast cancer that spreads to and forms a metastatic tumor in the lung is metastatic breast cancer, not lung cancer.
Under a microscope, metastatic cancer cells generally look the same as cells of the original cancer. Moreover, metastatic cancer cells and cells of the original cancer usually have some molecular features in common, such as the presence of specific chromosome changes.
Treatment may help prolong the lives of some people with metastatic cancer. In general, though, the primary goal of treatments for metastatic cancer is to control the growth of the cancer or to relieve symptoms caused by it. Metastatic tumors can cause severe damage to how the body functions, and most people who die of cancer die of metastatic disease.
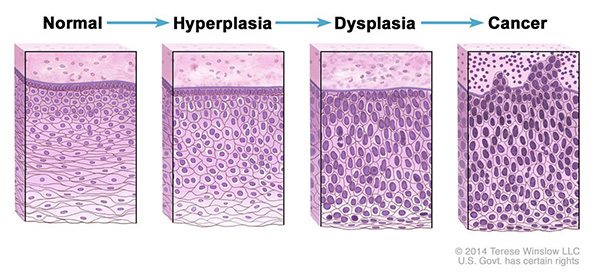
Tissue Changes that Are Not Cancer
Not every change in the body’s tissues is cancer. Some tissue changes may develop into cancer if they are not treated, however. Here are some examples of tissue changes that are not cancer but, in some cases, are monitored:
Hyperplasia occurs when cells within a tissue divide faster than normal and extra cells build up, or proliferate. However, the cells and the way the tissue is organized look normal under a microscope. Hyperplasia can be caused by several factors or conditions, including chronic irritation.
Dysplasia is a more serious condition than hyperplasia. In dysplasia, there is also a buildup of extra cells. But the cells look abnormal and there are changes in how the tissue is organized. In general, the more abnormal the cells and tissue look, the greater the chance that cancer will form.
Some types of dysplasia may need to be monitored or treated. An example of dysplasia is an abnormal mole (called a dysplastic nevus) that forms on the skin. A dysplastic nevus can turn into melanoma, although most do not.
An even more serious condition is carcinoma in situ. Although it is sometimes called cancer, carcinoma in situ is not cancer because the abnormal cells do not spread beyond the original tissue. That is, they do not invade nearby tissue the way that cancer cells do. But, because some carcinomas in situ may become cancer, they are usually treated.
Types of Cancer
There are more than 100 types of cancer. Types of cancer are usually named for the organs or tissues where the cancers form. For example, lung cancer starts in cells of the lung, and brain cancer starts in cells of the brain. Cancers also may be described by the type of cell that formed them, such as an epithelial cell or a squamous cell.
You can search NCI’s website for information on specific types of cancer based on the cancer’s location in the body or by using our A to Z List of Cancers. We also have collections of information on childhood cancers and cancers in adolescents and young adults.
Here are some categories of cancers that begin in specific types of cells:
Carcinoma
Carcinomas are the most common type of cancer. They are formed by epithelial cells, which are the cells that cover the inside and outside surfaces of the body. There are many types of epithelial cells, which often have a column-like shape when viewed under a microscope.
Carcinomas that begin in different epithelial cell types have specific names:
Adenocarcinoma is a cancer that forms in epithelial cells that produce fluids or mucus. Tissues with this type of epithelial cell are sometimes called glandular tissues. Most cancers of the breast, colon, and prostate are adenocarcinomas.
Basal cell carcinoma is a cancer that begins in the lower or basal (base) layer of the epidermis, which is a person’s outer layer of skin.
Squamous cell carcinoma is a cancer that forms in squamous cells, which are epithelial cells that lie just beneath the outer surface of the skin. Squamous cells also line many other organs, including the stomach, intestines, lungs, bladder, and kidneys. Squamous cells look flat, like fish scales, when viewed under a microscope. Squamous cell carcinomas are sometimes called epidermoid carcinomas.
Transitional cell carcinoma is a cancer that forms in a type of epithelial tissue called transitional epithelium, or urothelium. This tissue, which is made up of many layers of epithelial cells that can get bigger and smaller, is found in the linings of the bladder, ureters, and part of the kidneys (renal pelvis), and a few other organs. Some cancers of the bladder, ureters, and kidneys are transitional cell carcinomas.
Sarcoma

Sarcomas are cancers that form in bone and soft tissues, including muscle, fat, blood vessels, lymph vessels, and fibrous tissue (such as tendons and ligaments).
Osteosarcoma is the most common cancer of bone. The most common types of soft tissue sarcoma are leiomyosarcoma, Kaposi sarcoma, malignant fibrous histiocytoma, liposarcoma, and dermatofibrosarcoma protuberans.
Our page on soft tissue sarcoma has more information.
Leukemia
Cancers that begin in the blood-forming tissue of the bone marrow are called leukemias. These cancers do not form solid tumors. Instead, large numbers of abnormal white blood cells (leukemia cells and leukemic blast cells) build up in the blood and bone marrow, crowding out normal blood cells. The low level of normal blood cells can make it harder for the body to get oxygen to its tissues, control bleeding, or fight infections.
There are four common types of leukemia, which are grouped based on how quickly the disease gets worse (acute or chronic) and on the type of blood cell the cancer starts in (lymphoblastic or myeloid).
Our page on leukemia has more information.
Lymphoma
Lymphoma is cancer that begins in lymphocytes (T cells or B cells). These are disease-fighting white blood cells that are part of the immune system. In lymphoma, abnormal lymphocytes build up in lymph nodes and lymph vessels, as well as in other organs of the body.
There are two main types of lymphoma:
Hodgkin lymphoma – People with this disease have abnormal lymphocytes that are called Reed-Sternberg cells. These cells usually form from B cells.
Non-Hodgkin lymphoma – This is a large group of cancers that start in lymphocytes. The cancers can grow quickly or slowly and can form from B cells or T cells.
Our page on lymphoma has more information.
Multiple Myeloma
Multiple myeloma is cancer that begins in plasma cells, another type of immune cell. The abnormal plasma cells, called myeloma cells, build up in the bone marrow and form tumors in bones all through the body. Multiple myeloma is also called plasma cell myeloma and Kahler disease.
Our page on multiple myeloma and other plasma cell neoplasms has more information.
Melanoma
Melanoma is cancer that begins in cells that become melanocytes, which are specialized cells that make melanin (the pigment that gives skin its color). Most melanomas form on the skin, but melanomas can also form in other pigmented tissues, such as the eye.
Our pages on skin cancer and intraocular melanoma have more information.
Brain and Spinal Cord Tumors
There are different types of brain and spinal cord tumors. These tumors are named based on the type of cell in which they formed and where the tumor first formed in the central nervous system. For example, an astrocytic tumor begins in star-shaped brain cells called astrocytes, which help keep nerve cells healthy. Brain tumors can be benign (not cancer) or malignant (cancer).
Our page on brain and spinal cord tumors in adults has more information, as does our overview of brain and spinal cord tumors in children.
Other Types of Tumors
Germ Cell Tumors
Germ cell tumors are a type of tumor that begins in the cells that give rise to sperm or eggs. These tumors can occur almost anywhere in the body and can be either benign or malignant.
Our page of cancers by body location/system includes a list of germ cell tumors with links to more information.
Neuroendocrine Tumors
Neuroendocrine tumors form from cells that release hormones into the blood in response to a signal from the nervous system. These tumors, which may make higher-than-normal amounts of hormones, can cause many different symptoms. Neuroendocrine tumors may be benign or malignant.
Our definition of neuroendocrine tumors has more information.
Carcinoid Tumors
Carcinoid tumors are a type of neuroendocrine tumor. They are slow-growing tumors that are usually found in the gastrointestinal system (most often in the rectum and small intestine). Carcinoid tumors may spread to the liver or other sites in the body, and they may secrete substances such as serotonin or prostaglandins, causing carcinoid syndrome.
Credit: National Cancer Institute.
Subscribe to:
Comments (Atom)